
Ultrasound Course Module 4
First and Second Trimester Scanning
Lesson 2: Second/Third Trimester Obstetrical Ultrasound
- Guidelines
AIUM Practice Guideline for the Performance of Obstetric Ultrasound Examinations, American Institute of Ultrasound, 1 October 2007
For a complete list of guidelines see www.aium.org under above reference. -
Performance Objectives
Normal placentation without previa.
Posterior placenta previa.- Placenta/Cord Insertion/Cervix/Fluid
- Placenta Grade 0
- Smooth chorionic surface
- Homogenous echo texture
- Placenta Grade I
- Subtle irregularities of chorionic surface
- Scant, randomly dispersed echodensities
- Placenta Grade II
- More marked irregularity of chorionic surface
- More echodensities, more "organized" especially at basal surface
- Placenta Grade III
- Marked indentations on chorionic surface
- Marked, organized echodensities
- "Outlining" of cotyledons
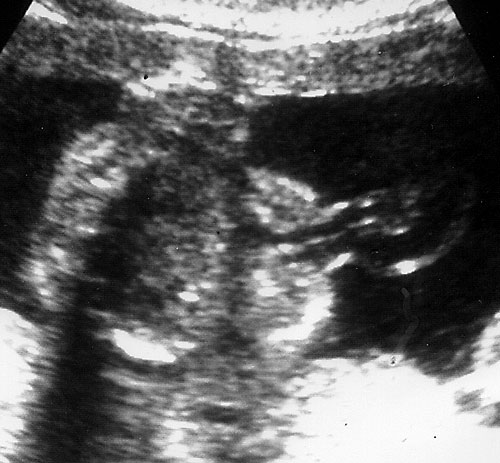
- Placental Cord Insertion Site
Note normal cord insertion into fetal abdomen without defect (left). Normal 3 vessel cord (right, at arrow). - Cervical Length by Transvaginal Ultrasound (TVS)
- Normal cervical length > 3 cm
Normal appearing cervix. Closed and long.
Length cervical canal
10-50 mm in 2nd and 3rd trimesters
50th% is 3.5 cm
10th% is 2.5 cm
90th% is 4.5 cm
- Cervical length < 2.5 cm at 22-24 weeks 6x increase in PTB before 35 weeks.
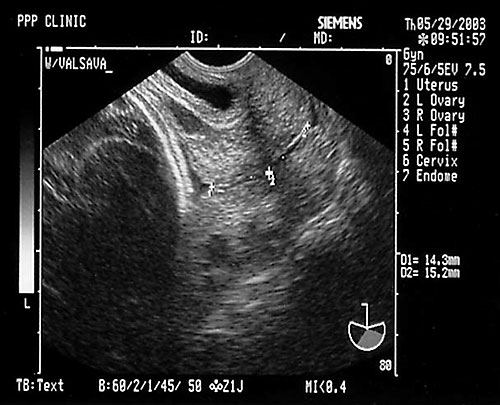
Shortening of cervix with mild funneling.- Often see shortening with bleeding/contractions/multiple gestation with delivery < 32 weeks
- Cervical length 1.8-2.0 cm best positive predictive value.
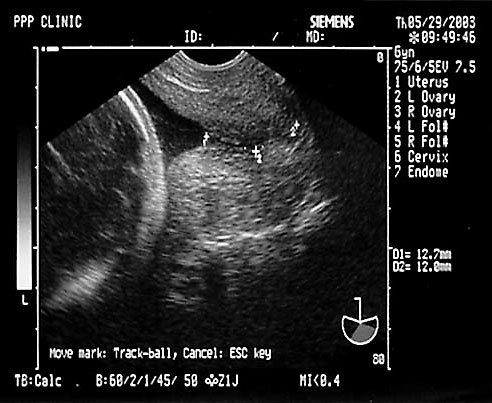
Marked funneling of cervix with shortening.- Cervical length 3.0 cm excludes preterm labor
- Cervical length 3.0 cm excludes preterm labor
- Problems with TVS for cervical length.
- Excessive pressure on probe
- Failure to empty bladder
- Use of transabdominal scan
- Normal cervical length > 3 cm
- Fluid
- Echo texture: not clinically significant.
- AF Volume is a balance of:
- Production (primarily renal/urinary)
- Resorption (primarily swallowing)
- Extrauterine loss (rupture of membranes)
- Amniotic Fluid Index (AFI)
- Measure of vertical measurement (centimeters) of deepest fluid pocket in each of four abdominal quadrants
- Saggital plane
- Measurement line should exclude umbilical cord/fetal parts
- Poor inter- and intra-rater reliability
- Measure of vertical measurement (centimeters) of deepest fluid pocket in each of four abdominal quadrants
-
Single Fluid Pocket >= 2 cm.
AFI pocket on ultrasound.- Must be demonstrable in at least two anatomic planes
- Subjective Assessment
- Polyhydramnios
- Associated with numerous conditions:
- Gestational Diabetes (especially with large fetus)
- Tracheo-esophageal fistula/atresia/obstruction
- Neural tube defects
- CNS abnormalities
- Isoimmuninzation/Hemolysis
- Twin-twin transfusion syndromes
- Aneuploidies (? secondary effect of decreased swallowing)
- > 50% idiopathic (no identifiable pathology).
- Increased Suspicion:
- Sudden dramatic increase in fundal height
- AFI > 22
- Any single fluid pocket > 8 cm deep
- Indication for comprehensive studies.
- Associated with numerous conditions:
- Oligohydramnios
- Associated with:
- Rupture of membranes
- Tamponade effect: normal AFI does not rule out Spontaneous Rupture Of Membranes (SROM)
- Uteroplacental insufficiency (especially Pregnancy Induced Hypertension (PIH) and post-dates)
- Intrauterine Growth Retardation (IUGR)/Small for Gestational Age (SGA)
- Renal or urinary tract abnormalities
- Heart failure (Fetal Demise)
- Aneuploidies (? secondary effect due to renal dysplasia)
- Increased Suspicion:
- AFI < 6
- No single pocket > 2 cm
- Very difficult sonographic imaging.
- Extremely difficult anatomic survey, especially soft tissue structures
- Indication for comprehensive studies.
- Associated with:
- Biophysical Profile (BPP) Testing
- Clinical Significance
- Screening test for uteroplacental insufficiency
- Chronic hypoxemia/acidosis
- 30 minutes maximum study duration.
- Five variables, two points each, score 0-10
- Breathing movements — 30 seconds of activity.
- Gross body movements — at least three discrete movements.
- Fetal tone — at least one flexion/extension movement.
- Reactive NST.
- Amniotic Fluid Volume — at least one, 2 cm vertical fluid pocket, demonstrable in two anatomic planes.
- Five variables, two points each, score 0-10
- Clinical significance of BPP.
BPP Score Risk of IUFD within 7 days 10/10 1/1000 8/8 (NST not done) 1/1000 8/10 (w/normal fluid) 1/1000 8/10 (-2 for oligohydramnios) 89/1000 6/10 (w/normal fluid) statistically equivocal 6/10 (with oligohydramnios) 89/1000 4/10 91/1000 2/10 125/1000 0/10 600/1000
- Clinical Significance
- Echo texture: not clinically significant.
- Placenta Grade 0
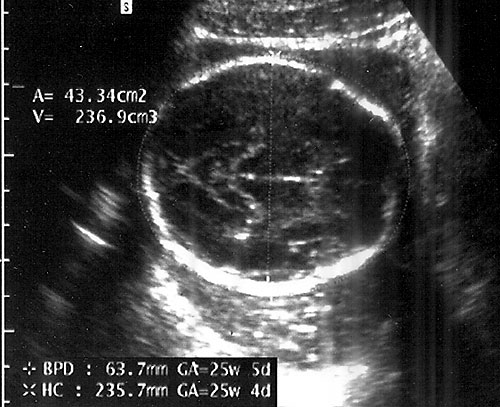
- Biparietal Diameter (BPD)/Head Circumference (HC)/Intracranial Anatomy — Ventricles/Atria/Posterior Fossa
- Accuracy is inversely related to gestational age: "one-two-three rule".
Measurements from outer edge at superior margin to inner margin at inferior margin to correct for fetal skull thickness (left). Proper measurement of head circumference (right). - Clinically meaningless, unless multiple parameters are measured and evaluated.
Normal transcerebellar and posterior fossa measurements.- Discard anomalous or asymmetric measures
- Carefully evaluate reliability of LMP
- Transcerebellar diameter: relatively insensitive to abnormal growth — in the absence of early dating ultrasound, always consider possibility of abnormal growth. (Hill LM, Guzick D, Fries J, Hixson J, Rivello D. Transverse cerebellar diameter in estimating gestational age in the large for gestational age fetus. Obstet Gynecol 1990;75:981-85. & Hill LM, Guzick D, Rivello D, Hixson J, Peterson C. The transverse cerebellar diameter cannot be used to assess gestational age in the small for gestational age fetus. Obstet Gynecol 1990;75(3 Part 1):329-33.)
- Measuring BPD/HC
- Axial plane at level of septum cavum pellucidum and thalamic nuclei. (Shepard M, Filly RA. A standardized plane for bieparietal diameter measurement. J Ultrasound Med 1982;1(4):145-50.)
Normal BPD at level of thalami with cavum seen. - Falx: midline and perpendicular to angle of insonation. (Simpson GF, Filly RA. Comparison of fetal head circumference measurements using standard and long linear array transducers. J Diagn Med Sonogr 1988;4:2)
Normal appearing posterior fossa (normal size<1.0 cm from vermis of cerebellum to occipital bone inner edge).
- Axial plane at level of septum cavum pellucidum and thalamic nuclei. (Shepard M, Filly RA. A standardized plane for bieparietal diameter measurement. J Ultrasound Med 1982;1(4):145-50.)
- Accuracy is inversely related to gestational age: "one-two-three rule".
- Neck — rule out thyromegaly/masses.
Normal appearing lips without clefting. - Face/lips/palate — view face to look at eyes, upper lip, palate and nose.
- Multiplanar views with coronal views of face through nose/lips. (Pretorius DH, Nelson TR. Three dimensional ulstrasound in gynecology and obstetrics. Ultraound Q 1998;14:218-233.)
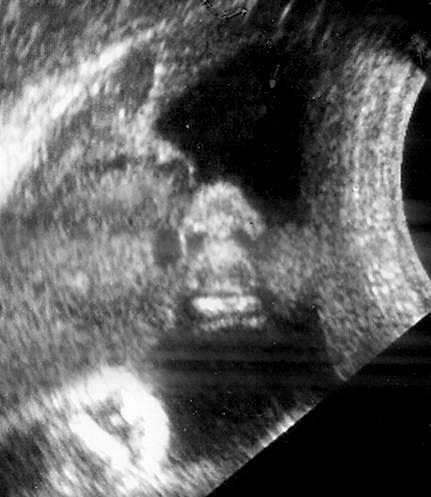
Normal nose and lips seen in coronal "swimmers view". - Sagittal view of face to visualize profile.
Normal sagittal view of fetal face.
- Views through axial plane to note palate/tooth buds.
Normal transverse view of palate at 18 weeks at level of tooth buds (left, at arrow). Normal fetal orbits seen to left of arrow in photo (middle). Normal ear just for fun (right)!
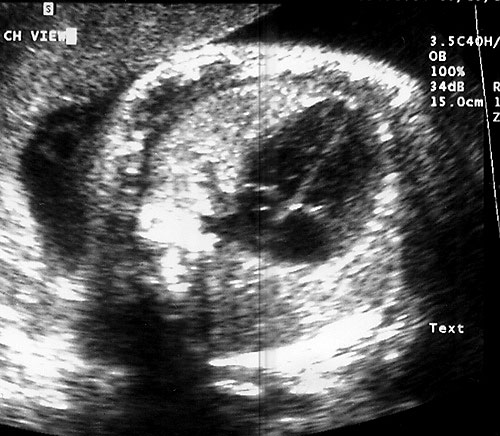
Normal 4-chamber heart view. - Multiplanar views with coronal views of face through nose/lips. (Pretorius DH, Nelson TR. Three dimensional ulstrasound in gynecology and obstetrics. Ultraound Q 1998;14:218-233.)
- 4 CH and left ventricular/right ventricular outflow tracts.
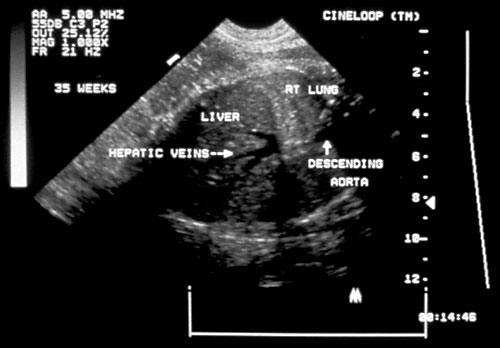
- Diaphragms — visualize in sagittal plane.
Normal diaphragm seen below right lung and above the liver in the middle of the picture with the hepatic veins diving below diaphragm. - Abdominal circumference.
- Stomach (size/position on left)
- Abdomen (cord insertion/bowel)
- Measurement:
Normal abdominal anatomy at level of abdominal circumference (left). DV=ductus venosus, LPV=left portal vein, RPV=right portal vein, S=stomach. Normal abdominal circumference with perpendicular measurements (right). Note measuring from spine to anterior abdominal wall and then perpendicular to first measurement. Many new machines now use a circumference function with an ellipse to place on the circumference.- Landmarks: stomach, portal vein and kidneys. (Chinn DH, Filly RA, Callen PW. Ultrasonic evaluation of fetal umbilical and hepatic vascular anatomy. Radiology 1982;144(1):153-7.)
- Axial plane (oblique planes generate wild errors).
- Most reliable single predictor of fetal weight.
- Least reliable correlate of gestational age.
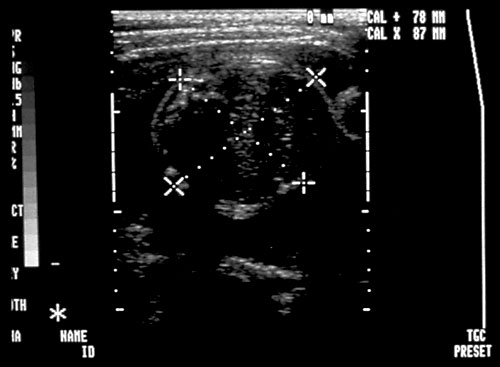
- Kidneys — look for renal pyelectasis (renal pelves > 4mm less than 20 weeks or > 1 cm after 28 weeks)
Normal appearing kidneys in transverse orientation (left). Normal sagittal view of kidney (right).
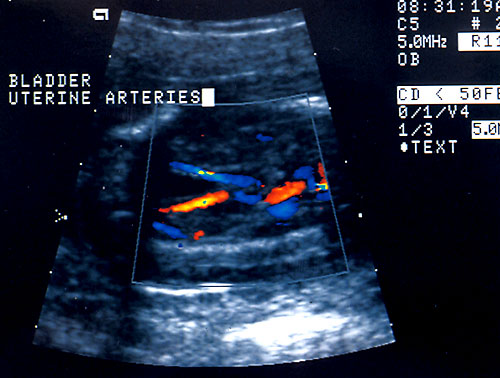
- Bladder
Normal fetal bladder at 18 weeks (left, at arrow). Lovely picture of both uterine arteries around normal bladder (right). This color flow picture documents the presence of the 3 vessel cord with the demonstration of the two uterine arteries coursing around the bladder. - Spine (need two perpendicular views)
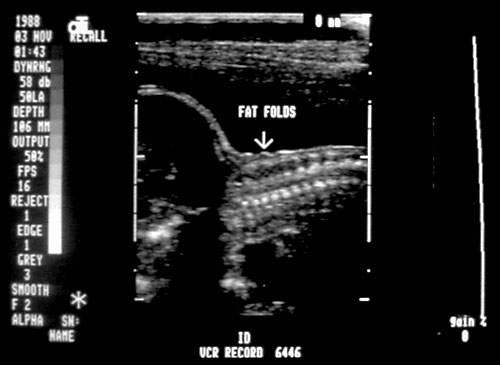
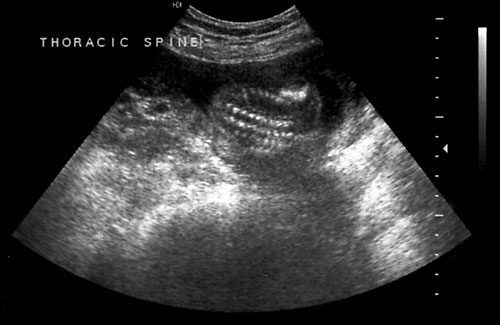
Normal cervical spine at 18 weeks (1). Another normal sagittal view of cervical spine seen in third trimester with folds of fat seen (2). Normal thoracic spine at 18 weeks (3). Normal sagittal view of lumbosacral spine at 18 weeks (4). Normal transverse view of lumbosacral spine at 18 weeks (5). - Extremities (hands/feet)
Normal fetal hand with four fingers and thumb on right side of photo (left). Normal fetal feet with five digits on each with normal anatomy (right).- Femur length — accurate for measuring gestational age.
- Most accurately measured perpendicular to angle of insonation. (Goldstein RB, Filly RA, Simpson G. Pitfalls in femur length measurements. J Ultrasound Med 1987;6(4):203-7. & Jeanty P, Rodesch F, Delbeke D, Dumont JE. Estimation of gestational age from measurements of fetal longg bones. J Ultrasound Med 1984;3(2):75-9.)
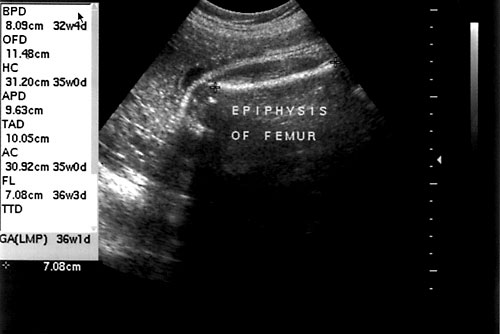
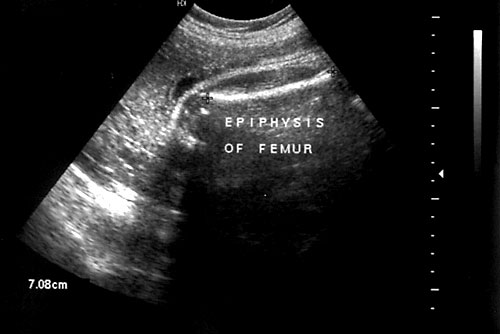
Proper measurement of femur. - Distal epiphysis not included in measurement. (Mahony BS, Filly RA. High-resolution sonographic assessment of the fetal extremities. J Ultrasound Med 1984;3(11):489-98. & Abrams SL, Filly RA. Curvature of the fetal femur: A normal sonographic finding. Radiology 1985;156(2):490.)
Femur at 36 weeks with epiphysis seen to left of photo at arrow.
- Most accurately measured perpendicular to angle of insonation. (Goldstein RB, Filly RA, Simpson G. Pitfalls in femur length measurements. J Ultrasound Med 1987;6(4):203-7. & Jeanty P, Rodesch F, Delbeke D, Dumont JE. Estimation of gestational age from measurements of fetal longg bones. J Ultrasound Med 1984;3(2):75-9.)
- Evaluate feet for clubbing and hands for position with phalanges.
- Femur length — accurate for measuring gestational age.
- Genitalia (visualize them if possible)
Normal male genitalia (1). Normal female genitalia (2). Bilateral fetal scrotal hydroceles in utero (normal variant) (3).
- Placenta/Cord Insertion/Cervix/Fluid





























- Manning FA, Platt LD, Sipos L. Antepartum fetal evaluations: Development of a fetal biophysical profile score. Am J Obstet Gynecol 1980;136(6):787-95.
- Baskett TF, Fray JH, Prewett SJ, Young LM, Allen AC. Antepartum fetal assessment using a fetal biophysical profile score. Am J Obstet Gynecol 1984;148(5):630-3.
- Manning FA, Morrison I, Lange IR, Harman CR, Chamberlain PF. Fetal assessment based on fetal biophysical profile scoring: Experience in 12, 620 referred high risk pregnancies: I. Perinatal morbidity by frequency and etiology. Am J Obstet Gynecol 1985;151(3):343-50.
- Manning FA, Morrison I, Harmon CR, Lange IR, Menticoglou S. Fetal assessment based on fetal biophysical profile scoring: Experience in 19,221 referred high risk pregnancies: II. An analysis of false-negative fetal deaths. Am J Obstet Gynecol 1987;157(4 Part 1):880-4.
- Baskett TF, Allen AC, Gray JH, Young DC, Young LM. Fetal biophysical profile and perinatal death. Obstet Gynecol 1987;70 (3 Part 1):357-60.
- Manning FA, Harman CR, Morrison I, Menticoglou S. Fetal assessment based on fetal biophysical profile scoring: III. Positive predictive accuracy of the very abnormal test (biophysical profile score=0). Am J Obstet Gynecol 1990;162(2):398-402.
- Manning FA, Harman CR, Morrison I, Menticoglou SM, Lange IR, Johnson JM. Fetal assessment based on fetal biophysical profile scoring: IV An analysis of perinatal morbidity and mortality. Am J Obstet Gynecol 1990;162(3):703-9.
